This week I was in the ultrasound department at the Western General. I had previously worked in an ultrasound department as an assistant so knew what to expect.
The week mainly consisted of obstetrics, and gynecological examination with a little general ultrasound. Through out the week I observed a number of gynecological examinations on women who were perimenopausal and post menopausal. One of the main difficulties I had with these examinations was identifying the ovaries. I generally found it difficult to pick out the ovaries in pre-menopausal women but found it increasingly difficult and sometimes nearly impossible on women who were of peri and post menopausal years. Another issue with this type of exam was that the anatomy changes with women who have had a hysterectomy.
One of the more interesting cases I dealt with was a patient who attended the department for a kidney scan due to a condition called Birt-Hogg-Dube syndrome (BHD). I had never heard of this condition and asked the patient all about it. He went on to tell me he had previously had a pneumothorax and his doctor had heard a crackling in his chest. He was then sent to a cardiologist because they suspected the crackling was coming from his heart. On investigation they could not find anything wrong with his heart and continued with more tests. On further investigation it was found that the patient had tumours in both kidneys, and tests revealed BHD syndrome. This led to him undergoing a partial bi-lateral nephrectomy. The patient was on a follow up appointment checking for any reoccurrence of tumours in his kidneys. This patient had no previous skin lesions and the condition was only identified due to him having a pneumothorax.
After further research I discovered that Birt-Hogg-Dubé (BHD) syndrome is a hereditary condition that was originally identified as a skin condition by three Canadian doctors. They found certain kinds of skin lesions on the faces and necks of several members of an extended family. In recent years, more symptoms have been linked to this syndrome, namely lung collapses and kidney cancer.
BHD syndrome is caused by mutations in the folliculing gene (FLCN). People who have the mutated gene may have lung cysts or experience collapsed lungs, and may develop kidney cancer. There is no typical BHD patient.
People with BHD syndrome may have none, one, or all of the physical symptoms associated with the condition. The fact that kidney cancer can be one of the symptoms of this syndrome makes it potentially serious. However, only a small percentage of those with BHD actually develop kidney cancer.
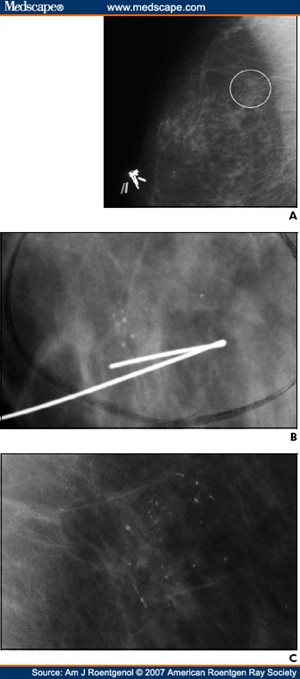
Attached to this piece of writing are images of BHD syndrome.

http://www.nature.com/jid/journal/v128/n1/full/5700959a.html
Article from the journal of investigative dermatology.