This was my first week of a two week elective placement. On arrival to the department I was introduced to staff and shown round by the superintendent. I had been looking forward to this placement and was happy with the schedule that had been arranged for me during my visit. I had specifically requested I would like some hands on with any A & E patients.
It took me a few days to familiarise myself with the systems and equipment, as every room had different types. The department has designated areas for different patients. For my first week I was placed in the rooms which are specifically for A & E and ward patients. I found it all a bit overwhelming at first as the radiographers do almost everything. When a patient arrives from A & E or a ward, the radiographer enters their details and examinations required into the system, after checking their previous history and justifying the examination. They then proceed with the request and then post process the details when finished. Every exposure taken is recorded in detail. They are written on the back of the patients’ request card, the card is then scanned into the system. The exposures are recorded once again during the post processing.
I expected things to be different here but I wasn’t quite prepared for just how different everything was. The equipment here is quite dated such as a Siemens Polydoros 80s which, luckily, I have used previously.
Protocols at the Perth Royal Infirmary are also very different as each orthopaedic surgeon has their own preferences of what views they would like for each examination. So if you have a patient who has had a knee replacement you have to refer to the consultants’ lists and see which views he requests before you perform the examination. Once I understood the procedures and protocols I found this to be a very good system of working.
The A&E patient list wasn’t as exciting as I initially thought. However there were lots of post operative patients arriving from the wards and this gave me the opportunity to practice horizontal beam laterals (HBL). In the past I haven’t had much of an opportunity to have hands on practice for this type of examination. It is performed at Queen Margaret Hospital, using the air gap technique with the up-right bucky for trauma patients with a suspected neck of femur fracture. Here they perform their HBL without the air gap technique but the principals are the same. This examination is performed on patients who are post operative, trauma and some orthopaedic clinic reviews. I was given the chance to perform a few and through practice I found them not as difficult as I initially thought.
My other experience this week was performing an examination on a patient coming in through A&E with a suspected dislocated shoulder. The examination was quite difficult due to the patients’ pain, although the pain relief began to work and I was able to assist with the views needed. Once the examination was finished I was allowed to return with the patient to the resuscitation unit at A&E and observe while the doctor manipulated the shoulder back into position. It took a doctor and 2 nurses to perform the manipulation. While the doctor was pulling the patients arm down and away from the patients body, one nurse has a bed sheet placed around the top of the patients arm to pull the shoulder up, with the other nurse held the patient on the bed. After a few minutes of pulling, you were able to hear the patients arm slide back into position.
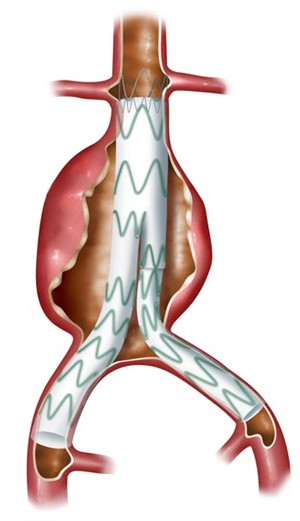
Attached to this piece of writing are images of fractured neck of femur and a hip replacement. A patient with a suspected fracture or a new replacement requires a HBL to show positioning of the fracture or replacement. There are also images of shoulder dislocations.