Week 10 Year 3
This week I was in the Royal Hospital for Sick Kids (RHSC). I had expected this week to be particularly challenging due to the different skills and techniques required while working with children. Being a mother I found myself acutely aware of the thoughts and feelings that some of the children and parents were experiencing.
There were difficulties involved in performing examinations on children while the parents were in the room, especially when the examination required immobilisation and the child was very young. I was constantly aware that I had to display professionalism and confidence in order to gain the trust of the parents, however it was a few days into the week before I was familiar enough with the environment to relax.
Over the week I encountered a number of children with medical conditions that were new to me. One patient I performed a knee examination on suffered from a condition called Dystonia (Sigawa syndrome). This condition is a rare genetic disorder which is characterised by an uncoordinated or clumsy manner of walking and dystonia. Dystonia is a general term for a group of muscle disorders generally characterised by involuntary muscle contractions that force the body into abnormal, sometimes painful, movements and positions.
The request card for this patient advised she had a previous diagnosis of dystonia in her feet, and was now experiencing the inability to straighten her left knee unless she was asleep. I found this difficult to understand how this patient was able to have her knee straight while sleeping but was unable to straighten her knee when she was awake. I have since researched this condition for a better understanding.
Dystonia in Segawa syndrome usually affects the legs; however some children may first develop dystonia in the arms. In some cases, the symptoms of Segawa syndrome may become noticeably worse or more pronounced in the afternoon and evening than in the morning. The symptoms of Segawa syndrome usually become apparent around the age of six years. Children with this condition usually show a dramatic and sustained improvement when treated with a drug called levodopa. Levodopa is an amino acid that is converted to dopamine, a brain chemical that serves as a neurotransmitter. Dopamine is deficient in children with Segawa syndrome. The disorder is caused by mutations of the GCH-1 gene.
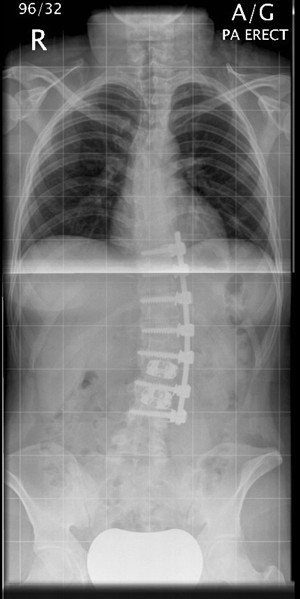
The RHSC is also the main centre for Paediatric and Young Adult Spinal Deformity (Scoliosis) in Scotland. During my time there I encountered a number of children attending for a spinal x-rays either pre-operative surgery on their spine or to review their condition to ascertain if there had been any changes in the degree of curvature to their spine. I found performing spinal examinations to be difficult. Mainly due to my lack of experience with this type of examination. I observed and assisted in a number of these examinations and gained a better understanding to what is evolved and the skills needed to produce a good image. It was not always clear by looking at some the children attending for a review x-ray that they had scoliosis until you had x-rayed them. I found it interesting to see how some children manage to compensate their posture to maintain what looks like a normal posture.
Overall my week at RHSC was very interesting and I encountered many new challenges and situations. The staff were very supportive and encouraging which helped to relax me in the new environment. I do feel, however, that I need much more experience in adapting techniques around babies and small children in order to gain confidence in this field. Attached to this piece of writing is an x-ray image of a child with scoliosis, this image is similar to images taken through the week.
http://members.optusnet.com.au/physio/scoliosis.html
A scoliosis is a lateral or sideways curve in the spine that is apparent when viewing the spine from behind.
http://www.nsd.scot.nhs.uk/services/specserv/spinaldeformity.html
Paediatric and Young Adult Spinal Deformity (Scoliosis) Scotland
 Print This Post
Print This Post